
According to Professor Michael Baum: “You cannot say that breast screening saves lives.” He has been arguing for decades that mammograms “do more harm than good.” He is not alone.
In 2017, The Conversation published an article ‘Routine mammograms do not save lives: The research is clear’. The article argued that there is no reliable evidence that routine mammograms for healthy women save lives and there is good evidence that such mammograms can cause harm.
The article was written by a Canadian Associate Professor of Nursing, Anne Kearney, who was part of a small group that started the breast screening programme in Newfoundland and Labrador. At the time of writing the article, Kearney had been looking at breast screening evidence for more than 20 years.
A few weeks later, The Conversation published a second article ‘Routine mammograms do save lives: The science’. This article was written by two Canadian authors: a Clinical Professor in the Department of Radiology and a Professor of Medical Biophysics and Medical Imaging.
“A recent article published by The Conversation Canada stated routine mammographies do not save lives – and that the harms of screening outweigh the benefits. As researchers who have worked in the field of breast cancer detection for decades, we know that exactly the opposite is true,” the two authors wrote.
In February 2014, the Swiss Medical Board released a report stating the evidence does not support a common medical mantra that mammograms are safe and capable of saving lives. It appears that mammography may prevent only one (1) death for every 1.000 women screened while causing harm to many more. In 2016, the Swiss Medical Board recommended no more systemic mammograms after reviewing all of the available evidence. Today, some regions in Switzerland have breast cancer screening programmes while others do not.
Around the time that the Swiss Medical Board was releasing its report, British breast-cancer specialist Professor Michael Baum was arguing, as he had for some years, that mammograms may shorten more lives than they extend.
In 2013, he published an essay in the British Medical Journal titled ‘Harms from breast cancer screening outweigh benefits if death caused by treatment is included’. In his essay, Prof. Baum attempted to estimate the harm of unnecessary treatment for breast cancer. He notes that radiation therapy, for example, increases women’s risk of lung cancer and heart failure. “I crudely estimate,” he writes, “that an addition of 1 to 3 deaths might be expected from other causes for every breast cancer death avoided.”
Further reading: Do Mammograms Kill More Women Than They Save? Scientific American, 13 October 2015
Prof. Baum is a veteran of world-class breast cancer research and treatment. He’s devoted his working life to uncovering the secrets of this all-too-common cancer and is now the Professor Emeritus of Surgery and visiting Professor of Medical Humanities at University College London.
Prof. Baum was originally one of three tasked with setting up the NHS Breast Screening Programme in 1987. However, after six or seven years of the start of the programme it became obvious to him that the benefits of screening had been grossly overestimated whilst the downside had been virtually ignored. Since then, he has become one of the most vociferous proponents for closing the programme down.
“Estimates of benefit have been grossly overestimated,” he explained to Liz Earle Wellbeing in 2019, “but none of the data shows that breast cancer screening reduces all-cause death. There was a modest effect on breast cancer death and no reduction in all-cause death, so you cannot say that breast screening saves lives.”
So how can screening reduce breast cancer deaths but not deaths of women overall?
“We now know that about 30% of breast cancers diagnosed by screening would never be life-threatening, but the treatment can kill you,’ Prof. Baum explained. Surgery, radiotherapy, chemotherapy and radiotherapy increases the risk of cardiovascular disease and even (rarely) lung cancer. “For every breast cancer death avoided there is one death caused by over-diagnosis.”
Read more: Professor Michael Baum: “You Cannot Say That Breast Screening Saves Lives,” Lize Earle Wellbeing, 4 October 2019
Let’s not lose touch…Your Government and Big Tech are actively trying to censor the information reported by The Exposé to serve their own needs. Subscribe to our emails now to make sure you receive the latest uncensored news in your inbox…
The Screening Paradox
The following is taken from Chapter 12 of Professor Michael Baum’s book ‘The History and Mystery of Breast Cancer’ as published by The Latte Lounge on 26 March 2020.
“The largest threat posed by American medicine is that more and more of us are being drawn into the system not because of an epidemic of disease but because of an epidemic of diagnoses. The real problem with the epidemic of diagnoses is that it leads to an epidemic of treatments. Not all treatments have important benefits, but almost all can have harms”
I’ve learnt to my cost over the last decade or so that whenever I write or speak about population-based screening for breast cancer by mammography, I must start with this disclaimer:
“I have devoted my life to improving women’s health, and I have been driven in part by the bad family history of breast cancer. Furthermore, I am one of the architects of the British National Health Service Breast Screening Programme (NHSBSP) and understand the theory and process of screening.”
In this chapter, I wish to explain the paradox of how, in good faith, I set up the service for the National Health Breast Screening Programme (“NHSBSP”) in the South East of England in 1998, and since then become one of the most vociferous proponents for closing it down. I want to conclude this chapter by suggesting that you, the readers, can do more for women’s health than anyone involved in running the NHSBSP.
In 1987, the Forrest report was published just two weeks before a general election called by Margaret Thatcher; it had sat on her desk for six months. This report was based on the review of all the available evidence that, included two randomised trials plus three case-control studies that predicted a 25% relative risk reduction (“RRR”) in breast cancer mortality favouring those who were invited to screening. (If the risk of something bad happening to you over, say, 10 years is 4%, then a RRR of 25% is a 1.0% reduction) It is noteworthy that little space was allocated to the potential harms of population-based screening by mammography.
Not surprisingly, the government of the day endorsed the recommendations and promised that if re-elected, a comprehensive screening programme involving women 50-65 who would be invited every three years for mammography would be established.
The NHSBSP was to be rolled out across the UK between 1988 and 1990. The service would be based on fixed screening units close to the population of high density and mobile units for remote areas.
These district units would feed into a select group of regional specialist centres in major hospitals that would be provided with additional facilities and manpower to handle the predicted surge in activity following the first round of screening.
At that time, I was a professor of surgery at Kings College Hospital, a major teaching hospital in South East London, caring for a socially deprived population. Dr Heather Nunnerly, head of diagnostic radiology, and I were given the dubious honour of setting up one of the first three centres in the country.
We were also given the task of setting up the training centre for all the clinicians, radiologists and radiographers who would staff the other units serving the South East of England as the programme was rolled out.
We were given 12 months to finish the job that was completed on time and on budget despite continuing with our full-time day jobs. I was proud of what we had achieved and, in good faith, accepted the evidence available at that juncture. I threw myself into my leadership role in the NHSBSP and was rewarded by being offered a seat on the National committee running the show.
My love affair with the NHSBSP was short-lived. Unlike most of the other members of the National Committee, I was directly involved in the day-to-day care of those women referred to me because of the activities on the front line of the screening programme. I found it very distressing to have to cope with otherwise well-women who had popped into the screening unit for a mammogram at the invitation of the Department of Health (“DOH”) whilst doing their grocery shopping in Butterfly Walk Mall and then found themselves labelled as cancer victims.
Worst of all was the unexpectedly high numbers diagnosed with duct carcinoma in situ (“DCIS”), a condition we rarely saw before screening began. Many of these cases were multifocal (scattered in little clumps all over the breast) and ended up with a mastectomy. How do you explain to a woman that she is “lucky” that we caught it “early” yet ends up having a mastectomy?
None of the DOH staffers or public health specialists on the National committee had to face the reality of these heart-breaking interviews. We were soon to learn that 20% of the cancers diagnosed in Butterfly Walk were DCIS, yet before we opened our doors, they amounted to less than 1.0% of our practice. I drew short-term comfort from this observation, assuming that in the fullness of time, this initial peak in the incidence of DCIS would be followed by a fall in the incidence of invasive breast cancer. I couldn’t have been more wrong.
Within a few more years, others noted that the “interval cancer” rates were far too high to achieve the predicted 25% reduction in cause-specific mortality. “Interval cancers” are those that appear as clinically detected lumps in the intervals between two invitations for screening examination.
These tend to be the fast-growing tumours that slip through the net. It rapidly became clear to me that we would never meet our targets, and there was no evidence for the predicted fall of invasive cancers following the mopping up of all these cases of DCIS. Furthermore, updated analyses of the evidence in the Forrest report, together with the publication of new trial reports, persuaded independent authorities to lower the estimate for the reduction in breast cancer mortality in a population-based screening programme from 25% to 15%.
After six or seven years into the programme, by which time it had been rolled out to the four corners of the UK, including the Islands and Highlands of Scotland, it became obvious to me that the benefits of screening had been grossly overestimated whilst the downside had been virtually ignored. Yet the letter inviting women into the NHSBSP remained unchanged, optimistic, pretty pink and frankly coercive.
Things came to a head for me in December 1994. The deputy chief medical officer called an emergency meeting of the NHSBSP national steering committee in the week between Christmas and the New Year. The meeting was convened to come up with a strategy to protect the programme in the face of the accumulation of adverse publications in the medical media.
I argued passionately for a revision of the false promises in the leaflet that went out with the invitations so that the lay public would at least be able to make an informed choice, as in my mind, it was a pretty close call to judge whether the benefits outweighed the harm.
I was a lone voice at the table, and the chairman summed up the opinion of the gathering as follows; “Professor Baum, if we include all this new information in the leaflets, then the women are unlikely to attend, and we will fail to reach our target of 70% uptake.” To which I replied, “If that is indeed the view of this committee, then I can no longer serve as I believe that women have the right to self-determination, I hereby resign and intend to make my feelings felt, but going public on the topic”.
True to my word, I published a long letter in the Lancet entitled ‘Screening for breast cancer; time to think and stop‘ a few months later. 25 years after the NHSBP was launched, the Department of Health was at last forced to set up an independent review that considered the adverse effects of screening; and to accept that women should no longer be denied the facts in helping them to decide whether to accept the call that was to be rewritten as an invitation and not like a summons.
Following that, a new information leaflet has been produced to accompany the invitation for screening that allows women to weigh up the balance of benefit versus harm so that they can reach an informed choice.
For every complex problem, there is an answer that is clear, simple, and wrong
It turns out that the clear and simple answer to the complex problem of breast cancer is wrong.
“Catch it early, save your life and save your breast” is a mantra that seems so self-evidently true that it is difficult for the lay public, and for that matter, many medically qualified NHS staff, to be willing to accept that the promise is false. There is, in fact, a modest in breast cancer mortality because of screening that is considered in the definitive publication from the Nordic Cochrane Centre. (See references)
In their booklet, they describe a synthesis of all the clinical trials that describe both the benefits and harms of screening using absolute rather than relative numbers, which makes it easier for lay people to comprehend.
Put in absolute terms, one can conclude that if 2,000 women are screened regularly for 10 years, they will benefit from the screening, as they will avoid dying from breast cancer.
The independent US Preventive Services Task Force derived a similar number in 2004. The NHSBSP prefer the figure one in 1,000 benefiting from screening, derived from a somewhat selective reading of the literature; whatever the agreed figure, the principles of this discussion remain the same.
However, even the figures one in 1,000 or one in 2,000 might be an overestimate. Remember, these data were derived from the trials that were mostly started in the 1970s and reported in the late 1980s. Since then, improvements in treatment, such as the adoption of tamoxifen and adjuvant chemotherapy, have narrowed the window of opportunity for screening, and we have witnessed a fall in mortality of 30–40%, both in the age group that are invited for screening as well as for the younger woman. Therefore, perhaps the correct number might be nearer to one in 3,000.
Whatever the number, that one woman who benefits from a decade of screening has a life of infinite worth, and if screening were as nontoxic as wearing a seatbelt, there would be no case to answer. However, there is a downside to screening, and that is the problem of over-diagnosis.
By this, I do not just mean the harms from false-positive results but the over-diagnosis of indolent disease, which includes the detection of cancer not destined to present clinically in that patient’s lifetime. This results from both the biology of the slow-growing tumours and the ageing woman dying because of other more common conditions.
It is deduced by the Cochrane report that for every life saved, ten healthy women will, because of screening, become cancer patients and will be treated unnecessarily. Again, the NHSBSP disputes this number but cannot deny the basic issue.
These women will have either a part of their breast or the whole breast removed, and they will often receive radiotherapy and sometimes chemotherapy. Five years ago, I did the sums to work out the balance between breast cancer deaths avoided by screening versus those lives lost from the rare toxic side effects following the treatment of over-diagnosed pseudo-cancers and published my results in the prestigious British Medical Journal (“BMJ”). (See references)
It appears that screening for breast cancer is a zero-sum game in that for every breast cancer death avoided; there was one death resulting from over-diagnosis. Of course, a clear majority of these over-diagnosed women would not die from treatment, but their quality of life would be seriously damaged, not to mention health insurance premiums. I’m not a maverick, as you will see if you check out the recommended information leaflet on screening produced by the independent Nordic Cochrane centre that is attached below or look at this decision aid prepared by the Harding Centre for Risk Literacy at the Max Planck Institute.
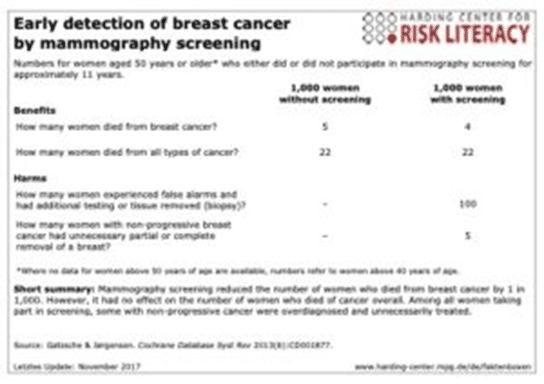
Let me run you through this. The table compares outcomes for 1,000 women screened and 1,000 women unscreened. There are 5 deaths from breast cancer in the un-screened group compared with 4 deaths from breast cancer in the screened group. That is what is meant by a 25% reduction.
Yet deaths from all cancers are the same, 22 in each case. If that is correct, then one cancer has been induced as a downstream effect or one cause of death has been misattributed.
5 women have been over-diagnosed with non-progressive breast cancers and had suffered the toxicity of unnecessary treatment. So, as I say, it’s a zero-sum game, yet the opportunity costs are huge-by that, I mean, the cost of the National programme might be better spent helping women with dementia, the most commonest cause of death for women over the age of 60 (see last chapter)
Breast Self-Examination (BSE)
Well, if mammographic screening cannot be recommended, surely BSE might save a few lives.
When things don’t turn out as planned in the management of breast cancer, there is a tendency to blame the victim! If the disease is too advanced for curative treatment at the point of diagnosis, it’s the patient’s fault for not checking herself regularly enough.
If the patient dies despite curative therapy, she is partly to blame for allowing it to grow to 3.00 cm when it might have been curable at 1.00 cm. Hence the shrill headlines in the women’s glossy magazines, “Catch it early, save your life and save your breast. Your life in your hands!”.
These features are usually accompanied by pictures of nubile young women demonstrating the “correct way” of doing BSE. This then reinforces the wrong message that young women get breast cancer. Sure, the youngest I’ve ever seen was 18 years old, and in my whole career, I think I’ve only seen about a dozen cases under the age of 30.
Breast cancer is predominately a disease of the post-menopausal years. Only 4% occur under 40, and the commonest age group is over 70.
At this point, I’ll play out a little charade with which I used to indulge myself when each group of new medical students joined my tutorial group.
1. “Why do we teach women to do BSE?”
Student A. “To catch it early, Sir”
1. “What do you mean by early?”
Student B. “When it’s small, Sir”
1. “Small is a metric of size, not of time. So, let me put it another way if you were a woman of, say 50, would you prefer your 1.0 cm tumour was 6 weeks old or a tumour the same size that was 6 years old?”
[Pause for thought…]
All students in unison. “6 years old, sir!”
1. “Correct, but stop calling me Sir. Indeed, if a cancer cell has grown to 1.0 cm in 6 weeks, it is very aggressive, but if it takes 6 years to appear, it is slow and indolent.
So how do we test whether BSE does save lives and breasts?”
Cheeky student C raises her hand. “Let’s do a clinical trial, Mike.”
- “I’d rather you called me Prof, but yes, you would do a clinical trial comparing women who were instructed in BSE and those who were not with the outcome measures of length of life and quality of life (“QOL”) accepting that breast surgery impairs quality of life.
- Have any such trials been conducted? [period of silence] Well, I didn’t really expect you to know, but the answer is yes, two such trials involving 10s of thousands of women.
- As you might have guessed already, the results were counterintuitive BSE does not save lives but double the number of futile biopsies for benign lesions, thus increasing the level of anxiety and impairing QOL. Ironically, I have no recall of ever seeing a woman in my clinic who claimed that her breast cancer was detected during her routine BSE.
- Most women are naturally aware of their bodies and these days are quick to report the chance observation of changes in the texture or shape of their breasts.
The Cochrane Collaboration, the greatest authority in the world for the evidence based in the practice of medicine, summarised the data as follows:
Regular self-examination or clinical examination for early detection of breast cancer.
Breast cancer is a common cause of cancer morbidity and mortality in women. Breast self-examination (examination of the breasts by the individual) or clinical breast examination (examination of the breasts by a doctor or a nurse) have been promoted for many years as screening methods to diagnose breast cancer at an early stage, to decrease the risk of dying from breast cancer.
This review searched for well-designed trials that assessed these methods and found two large population-based studies involving 388,535 women who compared breast self-examination with no intervention. The review of data from these trials did not find a beneficial effect of screening in terms of improvement in breast cancer mortality. The trials showed that women who were randomised to breast self-examination were almost twice as likely to undergo a biopsy of the breast, with 3,406 biopsies performed in the screening group compared to 1,856 biopsies in the control group.
The only large population-based trial of clinical breast examination combined with breast self-examination that was identified was discontinued.
Some women will continue with breast self-examination or will wish to be taught the technique. We suggest that the lack of supporting evidence from the two major studies should be discussed with these women to enable them to make an informed decision.
Women should, however, be aware of any breast changes. It is possible that increased breast awareness may have contributed to the decrease in mortality from breast cancer that has been noted in some countries. Women should, therefore, be encouraged to seek medical advice if they detect any change in their breasts that may be breast cancer.
(Regular self-examination or clinical examination for early detection of breast cancer (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.)
Should we de-implement screening?
In August 2018, I was invited to deliver a plenary lecture at a conference sponsored by the WHO, Oxford University and the British Medical Journal (“BMJ”). The theme of the conference was ‘Too Much Medicine‘, and I was speaking on the de-implementation of screening for cancer.
That’s right, you’ve read it correctly, the shutting down of screening programmes. I hope that is further evidence that I’m not a maverick when it comes to this subject. I started my talk by quoting from the book, “Thinking, fast and Slow” by the Nobel laureate Daniel Kahneman.
This book describes two systems of thought. System 1 is always ticking away in the background and provides effortless, intuitive solutions to problems. System 2 must be switched on to provide rational solutions to complex problems that make greater demands on cerebral activity.
This is an example lifted from his text: “A bat and a ball cost $1.10; the bat costs one dollar more than the ball. How much does the ball cost?” Your system 1 answer will be wrong; it is not 10 cents.
You must try harder to figure out the correct answer, 5 cents.
Breast cancer is a complex problem, and the “catch it early, save a life” mantra is a simple, intuitive answer that is wrong. To understand why it is wrong, you must energy your brain into type 2 thinking, which is too much effort for most lay people and politicians, however, compelling the data.
Screening for breast cancer is based on a simple mathematical model of the progress of cancer over time. In theory, DCIS comes first and, if left undetected, will progress to small invasive cancers under 1.0 cm.
If those are left undetected, then they will progress to 3.0, 4.0 and 5 cm. As time moves on, stage I cancers will become stage II cancers that will start spreading to present as stage III or IV cancers. If that is true, then the more cases of DCIS or very small invasive cancers you detect, the fewer stage II, III and IV cancers will appear. Sadly, that is not the case.
Once a country offers population screening, the incidence of DCIS and small stage I cancers shoot up, whilst the incidence of stage III and IV remains much the same. Furthermore, instead of a screening programme leading to an absolute reduction in mastectomy rates, the opposite is true.
These observations are so counterintuitive, and the effort to explain them is too much trouble; most government and healthcare agencies choose to deny these facts and slap them in the face. (“It is now as it was then as it may ever be, conceptions blind us to the facts that almost slap us in the face.” – Halsted, 1904 Bulletin of the Johns Hopkins Hospital. )
I look upon the screening debacle as a failed experiment conducted in good faith that has held back progress for more than 10 years. If the data don’t fit the hypothesis, then it’s time to change your mind. If you are willing to keep an open mind, all will be explained in chapter 14, ‘Time for a Paradigm Change‘, and the therapeutic consequences of this new conceptual model will appear in the last chapter.
So, what should women do in the meantime?
I often get to talk to patient support groups and even once addressed the formidable American advocacy group, The National Breast Cancer Coalition, in Washington, DC. Such groups are not hostile to the message and understand it all perfectly well, but I’m always asked what they should do if we abandoned screening. The simple answer would have been, “Who says you have to do anything? Forget about breast cancer and enjoy your life,” but that would appear less than diplomatic. So, what I say now is as follows:
- You can reduce your risk of breast cancer by keeping your weight down, getting plenty of exercise, eating lots of fruit and vegetables and keeping your alcohol intake down to no more than 7 units a week except for weddings, bar-mitzvahs and big birthdays.
- Don’t do ritualistic Breast Self-Examination (“BSE”) but be aware of changes in your body, such as the chance appearance of a dimple in the breast, distortion of the nipple or feeling of a lump. At that point, make an appointment with your doctor, don’t look upon it as an emergency, but for peace of mind, don’t postpone the visit for too long.
- Remember, there is more to life and death than breast cancer. Breast cancer no longer ranks in the top 5 causes of death for women. Consider the totality of your health and how you might avoid a premature death from more common conditions.
Furthermore, the breast screening units provide valuable resources for the diagnosis and treatment of breast cancer, and if we can identify a subgroup of women with a high risk of breast cancer and offer treatment that avoids the toxicity of radiotherapy (e.g. TARGIT/IORT), then the benefits might outweigh the cost.
Closing all the breast screening units might be throwing out the baby with the bathwater and, realistically, would never be accepted by politicians of any hue. This will be further explored in detail in the last chapter, ‘A new model of health care for women‘.
The Expose Urgently Needs Your Help…
Can you please help to keep the lights on with The Expose’s honest, reliable, powerful and truthful journalism?
Your Government & Big Tech organisations
try to silence & shut down The Expose.
So we need your help to ensure
we can continue to bring you the
facts the mainstream refuses to.
The government does not fund us
to publish lies and propaganda on their
behalf like the Mainstream Media.
Instead, we rely solely on your support. So
please support us in our efforts to bring
you honest, reliable, investigative journalism
today. It’s secure, quick and easy.
Please choose your preferred method below to show your support.
Categories: Breaking News, World News
Excellent article, and all true. A little known fact that mammogram screening actually significantly increases breast cancer risk.
This article makes no mention of the amount of radiation concentrated on the breast tissue during the mammography process. The accumulation of this radiation, over a number of screenings, risks creating cancer cells in the breast, that wouldn’t have occurred otherwise.As I understand it, the machines produced by the GE company, use many times more radiation than is required to perform it’s function.Consequently, I’ve ever had a mammography screening (I’m 61 years old). If women demand the continuation of screening, wouldn’t it be better to use thermal imaging machines instead ?
Or Ultrasound??
The effect of ultrasound on breast tissue is unknown. Few people are aware that the ultrasound scanning which is “routinely” used in pregnancy, has never been tested for safety. It has only been tested in it’s military capacity, for detecting submarines etc.Most people assume that if a procedure is being used in a medical capacity, it must have been tested by somebody, somewhere and found to be safe. This is not the case.Many decades ago, some research was carried out by a neurologist,(who’s name I can’t recall at present), who studied the effects on a baby’s developing brain tissue when exposed to ultrasound waves. She found that the tendency to focus the ultrasound on the baby’s head in order to measure it, concentrated the waves on an area of the brain related to attention span and language development. She proposed this as a possible cause of the huge surge in ADHD that was being seen at the time. She has since died, and her research, being inconvenient, has sadly died with her.She stated at the time, that no other safety studies had been carried out and I would assume that none have been done since. Anecdotally, I was aware of this research, before I became pregnant with my twins, 23 years ago. Therefore, I refused any ultrasound scans when I was pregnant. When my sons were 10 years old, I was told by their teacher, that they had a written and spoken vocabulary, that would be expected from an A grade 16 year old. Now, aged 23, they are both musicians and songwriters, one of them speaking 4 languages. I have no proof that the absence of ultrasound scanning has resulted in my sons being the way they are but it’s certainly worth noting. If there is a correlation, I mourn the repressed potential of a generation. One might almost imagine it was deliberate, but that would be a conspiracy theory, wouldn’t it ?
Just like regular colonoscopies do not prevent colon cancer, radiation from mammography does not save lives. Quite the opposite, it administers a healthy dose of radiation to the breast tissue. Our medical system in the USA is soooo screwed up. People getting fatter by the minute now being offered a new injectable weight loss product that paralyses the gut. Yes folks, please wake up. A healthy lifestyle is all the medicine you need.
Known for 20 years. Moreover, there are 20 cures for cancer your doctor will never tell you about and not one vaccine works, but every vaccine injures.
OH WOW!! What an eye opener…thank you so much!! m slowly dying now from Remdesivir poisoning. But can’t get anyone to help me. What SAD WORLD!
Have you reached out to Dr Pierre Kory, he has been helping thousands who are jab injured and hospital injured. Dr Peter McCullough is also helping people, they are both in the US. Im sorry this has happened to you, sending prayers for healing.